| Data Segment | Initial Code |
|---|---|
| There are no specialist doctors | lack of specialist doctors |
| Same medicine without proper check-up | inadequate treatment |
| Referred outside immediately | external referral |
| Machines do not work | equipment failure |
| Cannot measure BP | lack of basic equipment |
| Long waiting time | long waiting time |
| Medical center is far | distance barrier |
| Not enough privacy | lack of privacy |
| Not aware of services | lack of awareness |
| Avoid going unless urgent | avoid seeking care |
13 A Standard Qualitative Analysis Example
(PSY206) Data Management and Analysis
In this example, we demonstrate a standard qualitative research workflow, beginning with the formulation of a research problem and progressing through data collection, coding, theme development, memo writing, and interpretation.
Although presented in sequential steps for clarity, it is important to note that qualitative research is inherently iterative. Researchers often move back and forth between stages, refining earlier decisions in light of emerging insights.
13.1 Step 1: Research Design
Research Problem
We aim to understand:
What barriers do university students face in accessing healthcare from the Dhaka University Medical Center?
This is a qualitative research question, as it seeks to explore students’ experiences, perceptions, and interpretations rather than measure numerical relationships.
Research Approach
We adopt a qualitative descriptive approach, which is appropriate for obtaining a clear, practical understanding of a phenomenon in everyday terms.
- Focus: understanding student perceptions and experiences
- Goal: produce a rich, straightforward description of barriers
- No hypothesis testing or statistical inference
Sampling
We use purposive sampling, selecting participants who are likely to provide relevant and meaningful insights.
- Participants: 8 university students
- Selection basis: experience with the medical center
- Focus: information-rich cases rather than representativeness
Data collection continues until saturation, that is, when no substantially new insights or patterns emerge from additional interviews.
13.2 Step 2: Data Collection
Data are collected using semi-structured interviews, which allow participants to express their experiences in their own words while ensuring that key topics are consistently covered across interviews.
13.3 Raw Data (Interview Excerpts)
The following excerpts illustrate the type of qualitative data collected:
Participant 1:
“The medical center is affordable, but there are no specialist doctors. For serious problems, I go outside.”
Participant 2:
“Many of the machines do not work properly. Last time, they could not even measure my blood pressure.”
Participant 3:
“It is always crowded. I have to wait for a long time, so I avoid going unless it is urgent.”
Participant 4:
“I do not trust their treatment much. They usually give the same medicine without proper check-up.”
Participant 5:
“The medical center is far from my hall. When I am sick, I do not feel like going there.”
Participant 6:
“There is not enough privacy. It feels uncomfortable to talk about personal health problems.”
Participant 7:
“I am not sure what services are actually available there.”
Participant 8:
“The treatment is very basic. If the condition is serious, they refer you outside immediately.”
13.4 Step 3: Data Familiarization
Following data collection, we engage in data familiarization, which involves reading and re-reading the interview transcripts to develop a deep understanding of the content, context, and emerging patterns.
This step is essential because effective coding depends on a strong grasp of the data. At this stage, the researcher begins to notice recurring ideas, tones, and potential patterns, but does not yet formally assign codes.
It is important to note that qualitative analysis is iterative; insights gained during later stages may lead the researcher to revisit this step.
Initial Memo
Students repeatedly mention limitations in treatment, facilities, and trust. There is an early indication that the medical center is not perceived as reliable.
Memo writing begins at this stage and continues throughout the analysis. Memos serve as a record of analytical thinking and help bridge raw data and interpretation.
13.5 Step 4: Coding (Open and Axial Coding)
Coding is the core analytical process in qualitative research. It involves systematically organizing data into meaningful units and assigning labels (codes) that capture their essential meaning.
In this example, we follow a thematic analysis approach informed by grounded theory coding logic, moving from open coding to axial coding.
Identifying Data Segments
We first break the data into meaningful segments. Each segment represents a distinct idea or experience expressed by participants.
Examples include:
- “There are no specialist doctors”
- “Machines do not work properly”
- “Long waiting time”
These segments form the basis for coding.
Open Coding
Open coding is the initial stage of coding, where each data segment is examined and assigned a descriptive label.
At this stage:
- Coding is exploratory
- Some overlap or redundancy is acceptable
- The goal is to capture all relevant ideas
Memo (During Coding)
Several codes relate to treatment limitations and system inefficiency. These begin to cluster into broader concepts.
This memo reflects the early analytical insight that codes are not isolated but may form meaningful groups.
Axial Coding (Refining Codes)
Axial coding involves grouping related codes and refining them into more abstract categories. This step reduces redundancy and begins to reveal relationships among codes.
| Data Segment | Code |
|---|---|
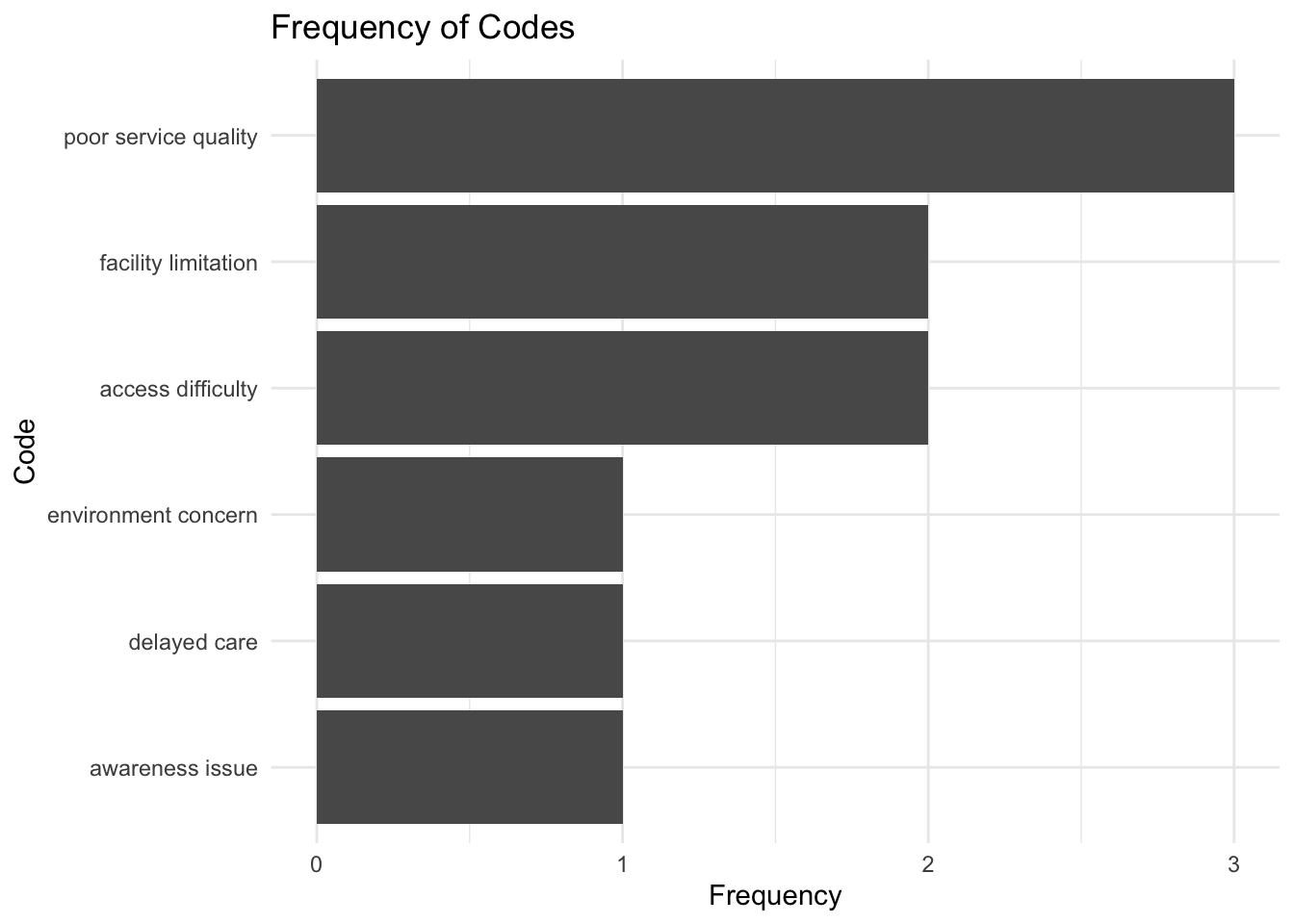
| No specialist doctors / Same medicine without proper check-up / Referred outside immediately | poor service quality |
| Machines do not work / cannot measure BP | facility limitation |
| Long waiting time / Medical center is far | access difficulty |
| Not enough privacy | environment concern |
| Not aware of services | awareness issue |
| Avoid going unless urgent | delayed care |
Through axial coding:
- Similar codes are merged
- Concepts become more abstract
- Relationships between issues begin to emerge
Memo (After Refinement)
“Poor service quality” appears as the central issue connecting multiple concerns such as lack of specialists and inadequate treatment.
This memo highlights the emergence of a core concept from the data.
Optional: Code Frequency Summary
Although qualitative research is not primarily concerned with quantification, simple summaries such as code frequency can provide a descriptive overview of patterns in the data.
13.6 Step 5: Developing Themes (Selective Coding)
At this stage, we group refined codes into broader themes. This corresponds to selective coding, where core patterns in the data are identified and organized.
Themes represent higher-level meanings that answer the research question.
Themes
Theme 1: Poor Quality of Medical Service
- poor service quality
Theme 2: Structural and Access Barriers
- facility limitation
- access difficulty
Theme 3: Awareness and Environmental Concerns
- awareness issue
- environment concern
Theme 4: Consequence: Delayed Care
- delayed care
Theme Mapping
| Theme | Code |
|---|---|
| Poor Quality of Medical Service | poor service quality |
| Structural and Access Barriers | facility limitation |
| Structural and Access Barriers | access difficulty |
| Awareness and Environmental Concerns | awareness issue |
| Awareness and Environmental Concerns | environment concern |
| Consequence: Delayed Care | delayed care |
Memo (Theme Level)
Barriers are interconnected. Service quality issues combine with access and awareness problems to shape student behavior.
This memo captures how different themes interact rather than exist independently.
13.7 Step 6: Interpretation
Interpretation integrates themes into a coherent explanation of the research problem.
Students face multiple barriers when accessing healthcare from the Dhaka University Medical Center. The most prominent issue is poor service quality, including lack of specialist doctors and inadequate treatment practices. Structural barriers such as malfunctioning equipment, long waiting times, and distance further discourage use. In addition, lack of awareness and privacy concerns reduce willingness to seek care. As a result, students often delay treatment or seek care elsewhere.
Interpretation must remain grounded in the data while providing a meaningful explanation of observed patterns.
13.8 Step 7: Trustworthiness and Reporting
Although presented as a final step, trustworthiness should be considered throughout the research process.
To ensure quality:
- Credibility: consistency of patterns across participants
- Dependability: systematic and transparent coding process
- Confirmability: findings grounded in the data rather than researcher bias
Final Memo
The medical center is perceived as a basic facility suitable mainly for minor issues. Improving service quality, accessibility, and communication may increase utilization.
13.9 Key Learning Points
- Qualitative research follows a structured but iterative process
- Coding evolves from open → axial → selective
- Themes capture patterns across data
- Memo writing supports continuous analytical thinking
- Interpretation must clearly connect findings to the research question